Modeling Infectious Disease Transmission Using GoldSim
Greg Paoli, and Todd Ruthman, Decisionalysis Risk Consultants (now Risk Sciences International), and Barry Michaels, The Michaels Group
(Orignally published in the GoldSim eNewsletter - Fall 2003)
Introduction
The need to better understand the transmission of infectious agents has been underscored by recent events including the international SARS crisis and reports of the considerable burden of disease associated with infections acquired in hospitals. Many questions remain regarding the best way to reduce transmission of infectious agents. The answers are of great interest to public health as well as to the health care, food service and consumer products industries.
The transfer of pathogens between patients and health care workers in a hospital is an important consideration in developing hospital policies and procedures. Hospitals may implement one or more mitigation strategies (e.g. gloves and other barriers, isolation of patients, hand hygiene products or procedures) to reduce the incidences of infection due to pathogen transfer. These mitigation strategies are implemented in a very complex and dynamic environment. Computer simulation of the transmission and mitigation processes can improve our understanding of exactly how the system generates and propagates risk and how to most effectively manage it.
This article discusses the use of GoldSim to model the transfer of pathogens between patients and health care workers in a hospital. The model generates simulated outbreaks in hospital wards, where the onset, extent of spread, and control of the outbreak is a manifestation of natural variability and the impact of simulated control strategies.
The Model
The following is a simplified description, focusing on the use of GoldSim to represent model elements, for some exploratory models. In modeling microbial agents, bacterial counts are commonly expressed as colony forming units (CFU). A new unit, CFU (colony forming unit) was created for the model.
Each patient and health care worker was represented by a reservoir with units of CFU. During a simulation run, each patient element might actually represent several individuals as patients were discharged and admitted. Each health care worker element might represent several individuals due to shift changes. Patient turnover was modeled using random Timed Events. Shift changes where modeled using regular Timed Events. Discharging patients and shift changes would reset the reservoir counts to zero. In one version of the model, new patients were assumed to be the initial source of the pathogens. Each new patient may have an initial pathogen count of zero or greater. A stochastic element was used to determine the initial pathogen count for each new patient. Each new health care worker was assumed to have an initial pathogen count of zero.
As the simulation run progressed, contact events between individual patients and health care workers could result in the transfer of pathogen from one to the other.
Contact between individual patients and health care workers were modeled using Timed Event elements with defined rates but random occurrences. Each contact event would trigger two Discrete Change Events: one from the patient to the health care worker and one from the health care worker to the patient. Each transfer was expressed in units of CFU, the amount of which depended on the current number of CFU in the respective reservoir (patient or health care worker).
Each patient reservoir was created with multiple discrete additions and withdrawals - one for each possible contact event. The number of CFU transferred from the health care worker was modeled as an addition, while the number of CFU transferred to the health care worker was modeled as a withdrawal. Health care worker reservoirs were also created with discrete events (in reverse, with patient withdrawals representing health care worker additions). Patient reservoirs also included a withdrawal rate to simulate the potential for a decline in the number of pathogens over time.
Results and Discussion
A sample result for a single patient is shown below:
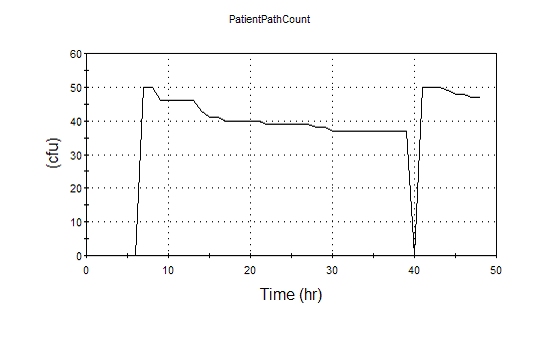
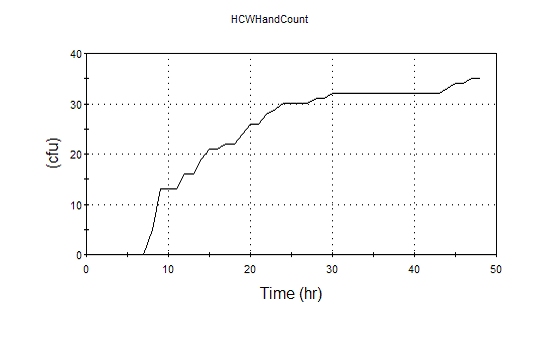
In this example, the new patient reservoir was assumed to have a starting population of 50 CFU. For simplicity in this example, no shift change occurred. The corresponding results for a single health care worker are shown below:
The model, using the dashboard elements to provide a user interface, provides the ability to simulate the behavior of patients and health care workers by controlling the statistical properties of their interaction using GoldSim model elements. The model generates simulated outbreaks in hospital wards, where the onset, extent of spread, and control of the outbreak is a manifestation of natural variability and the impact of control strategies.
The impact of various policies (including variability in compliance and efficacy) can be studied over many realizations to discover the underlying relationship between policy elements and risk reduction. Initial results suggest that variability in individual behaviors (e.g., individuals with a very low frequency of handwashing) can dominate the fate of outbreaks, suggesting that less importance should be assigned to the notion of average or typical behavior. This has implications for the measurement of performance and compliance in designing and evaluating infection control policies.
In applying GoldSim to this application, the user interface, stochastic elements, timed random events and the use of reservoir elements were found to be important tools to represent and study this infectious disease transmission system.